History of Present Illness: A woman in her 20’s presents to the ER for 2 days of RLQ pain with some radiation to her low back associated with nausea but no fever, diarrhea, dysuria, discharge or other complaints.
Vital Signs & Physical Exam: Vital signs are normal
Physical exam is otherwise normal except for slight RLQ tenderness
Initial Diagnostic Testing:
- CBC: normal except but CRP elevated at 16
- Chem-7: normal except
- UA: shows shows 100 WBC and 30 squammes, few bacteria
- Imaging: US shows dominant R ovarian follicle/cyst 1.6 cm in size and small, likely physiologic, free fluid. CT for appendicitis was negative
What is the most likely diagnosis?
- A) Ovarian cyst
- B) Mittleshmertz
- C) PID
- D) Ovarian torsion
SCROLL DOWN FOR ANSWERS & 1-MINUTE CONSULT
<<<<<<<<<<<<<<<<<<<<< ADVERTISEMENT & SPACER >>>>>>>>>>>>>>>>>>>>>
****************************************************************************
THE EMERGENCY MEDICINE POCKETBOOK TRIFECTA
Get one of our publications, all designed specifically for Emergency Care Providers:
- Emergency Medicine 8-in-1 Diagnostics & Procedure Guide, 5th edition (NEW)
- Emergency Medicine 1-Minute Consult Pocketbook, 5th edition (NEW)
- A to Z pocket EM Pharmacopoeia, 4th ed (NEW)
***************************************************************************
<<<<<<<<<<<<<<<<<<<<<<<<< END SPACER >>>>>>>>>>>>>>>>>>>>>>>>>
ANSWER:
- A) Ovarian cyst – usually painless if simple and <2.5cm
- B) Mittleshmerz – a diagnosis of exclusion and would need to know where she was in her cycle. Should be midcycle and rarely lasts more than a day
- C) PID – common and frequently presents with mild and/or atypical symptoms along with an unimpressive exam and CBC.
- D) Ovarian torsion – unlikely given size of follicle/cyst and clinical presentation
1-Minute EM Consult on the topic for this case from the Emergency Medicine 1-minute Consult Pocketbook
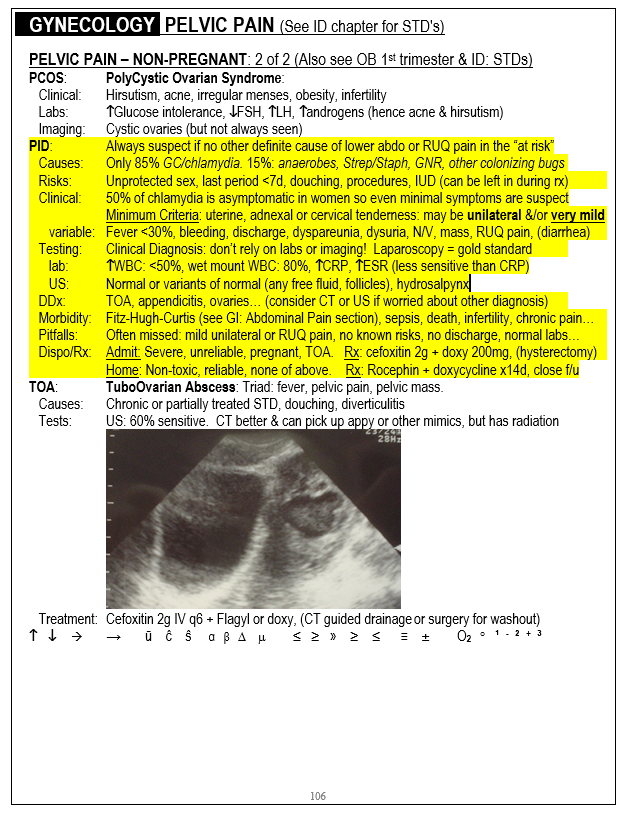
Click here for the free online em1minuteConsult page
CASE CONCLUSION: cath UA was normal, pelvic exam had mild milky discharge and slight CMT, chlamydia was positive
CASE LESSONS: Free fluid can be seen at any point in menstrual cycle but is most common in the 5 days prior to onset of menses. The fluid is thought to be due to increase capillary permeability from estrogen spiking rather than from ovulation itself