****
Gallbladder & RUQ Ultrasound – Pearls & Pitfalls:
- Know your limitations: Ultrasound may help clarify findings elicited by a thorough history and physical exam. When used correctly, it can greatly improve diagnostic accuracy, and help guide patient management, especially for time-critical diagnoses and treatment of unstable patients. It can also decrease the use of CT scan and thereby minimize radiation exposure. If you use ultrasound in your ED, you need to consider your skill level and know your limitations. When unsure, order a formal study. If your department has an ED dedicated ultrasound machine, it should consider implementing a quality improvement program that is approved by both ED administration and radiology.
- Finding the Gallbladder: Lying the patient on their left side and starting by locating the inferior liver edge can help.
- The Sonographic Murphy’s Sign: To check for a sonographic Murphy’s sign, which is a sign of cholecystitis, place the ultrasound probe at the maximal point of tenderness in the right upper quadrant. If the probe is placing direct pressure on the gallbladder fundus, you have a positive sonographic Murphy’s sign. False negatives may occasionally occur if the patient has received opiates prior to examination.
- The Gallbladder Wall: One sign of cholecystitis is a thickened gall-bladder wall. The normal gallbladder wall can be up to 3mm thick. The most common conditions other than cholecystitis that may cause thickening of the gallbladder wall include hepatitis, hypoalbuminemia, tumor, hyperplastic cholecystosis, adenomyomatosis, and CHF. The presence of pericholecystic fluid, in the absence of ascites also supports the diagnosis of acute cholecystitis. If there is clinical uncertainty, a nuclear biliary scan (HIDA or DESIDA scan) may be performed.
- The Common Bile Duct: A dilated common bile duct is another sign of acute cholecystitis. The normal common bile duct inner diameter should be less than 4mm, but may be higher, up to 10mm, post-cholecystectomy. In addition the diameter may be higher in older patients, up to 1mm per decade of life.
- The Gallbladder Contents: Look for a dilated gallbladder, evidence of stones, and for sludge. Gallstones should be mobile, unless they are impacted in the gallbladder neck, and should cast an acoustic shadow. If all stones are mobile in a patient who remains symptomatic, consider that they may be a red-herring and not the true cause of the patient’s pain. Remember that approximately 15% of adults have asymptomatic gallstones. If there are no sonographic signs of cholecystitis, but a gallstone is impacted (non-mobile) in the gallbladder neck, be suspicious for early cholecystitis and consider admission, additional imaging or at least next-day follow-up. Always also consider early cholecystitis when pain lasts for more than 6 hours, even when the ultrasound is normal except for the presence of a stone. Uncomplicated gallstone attacks usually should only last a few hours. Make sure to explain this to patients if you for some reason decide to send them home with opiates. Attacks lasting longer than that may be something more serious.
- Pitfalls: Don’t miss a single obstructing gallstone hidden in the gallbladder neck. It can sometimes be hard to see. Also, do not get faked out by an incidental “red herring” gallstone. As previously mentioned, many people have gallstones for years with no symptoms, so if everything does not fit clinically, look further for something else causing the abdominal, flank or rib pain. Some examples include aortic aneurysm, Fitz-Hugh-Curtis syndrome, high appendicitis, PE, kidney stone and pneumonia. Finally don’t miss a AAA, even if it is also incidental, because you did not look for it. Ultrasound techs look. The aorta is not that far away, and should be checked routinely in anyone over the age of 50 who is having an abdominal ultrasound for another reason. Screening saves lives!
*Want more educational images? Check out the ED Atlas on CD
****
Right Upper Quadrant Ultrasound

Single Mobile Gallstone: Beware! This can be associated with a resolved attack of biliary colic, but can also be a red herring in a patient suffering from a non-biliary emergency medical condition!
****

single stone hidden in gallbladder neck
****

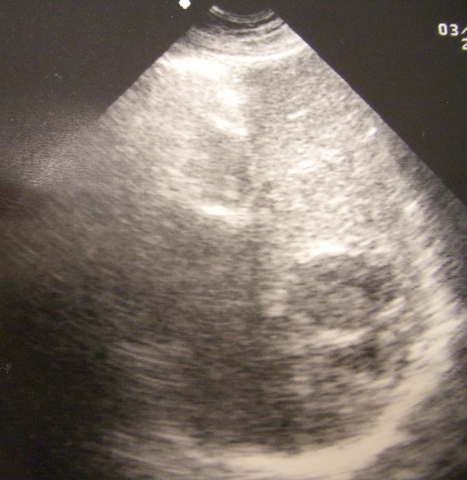
Cholecystitis with pericholecystic fluid
****

Liver Abscess

Liver Abscess
Liver Abscess
****

Cholecystitis with perforation and free air
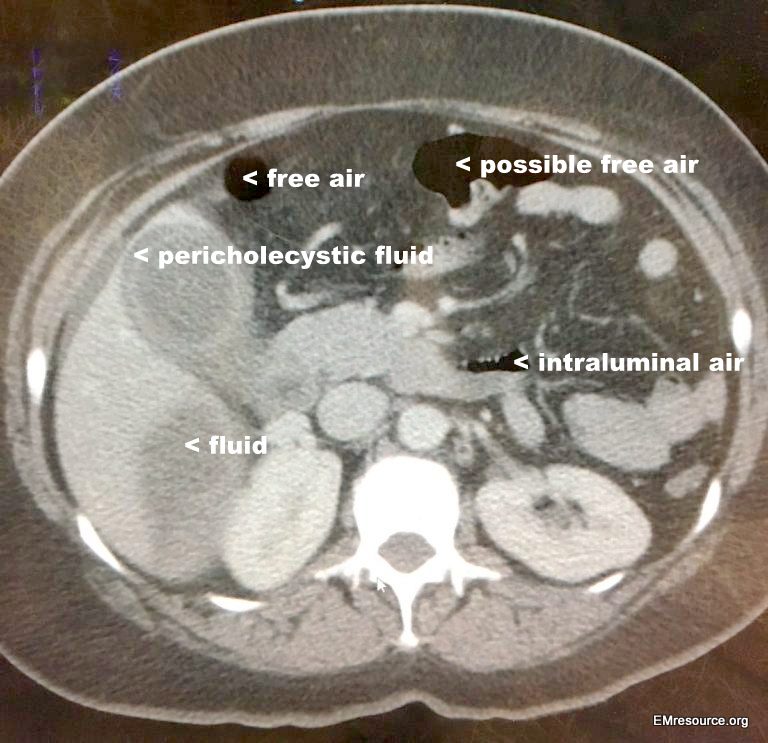
CT of patient above
****
Gallbladder & RUQ Ultrasound
– Polyps v. Stones:
- Mobility: Gallstones tend to be mobile if they are not impacted in the gallbladder neck, while polyps are non-mobile. If you image a gallstone that is not impacted it should settle to a dependent position with gravity. If you then reposition the patient, the gallstone will often settle into a new location. Polyps, on the other hand, are by their nature attached to the gallbladder wall and do not settle with gravity.
- Shadowing: Gallstones, unless they are very small, will cast an acoustic shadow. This is a type of ultrasound artifact where a thin sector type area far-field from of sonically dense object, such as a gallstone will appear completely black. See the comparison image. Polyps however are not dense enough to cast a shadow. Although they are echoic, some of the ultrasound waves still pass through and therefor, no shadow is cast.
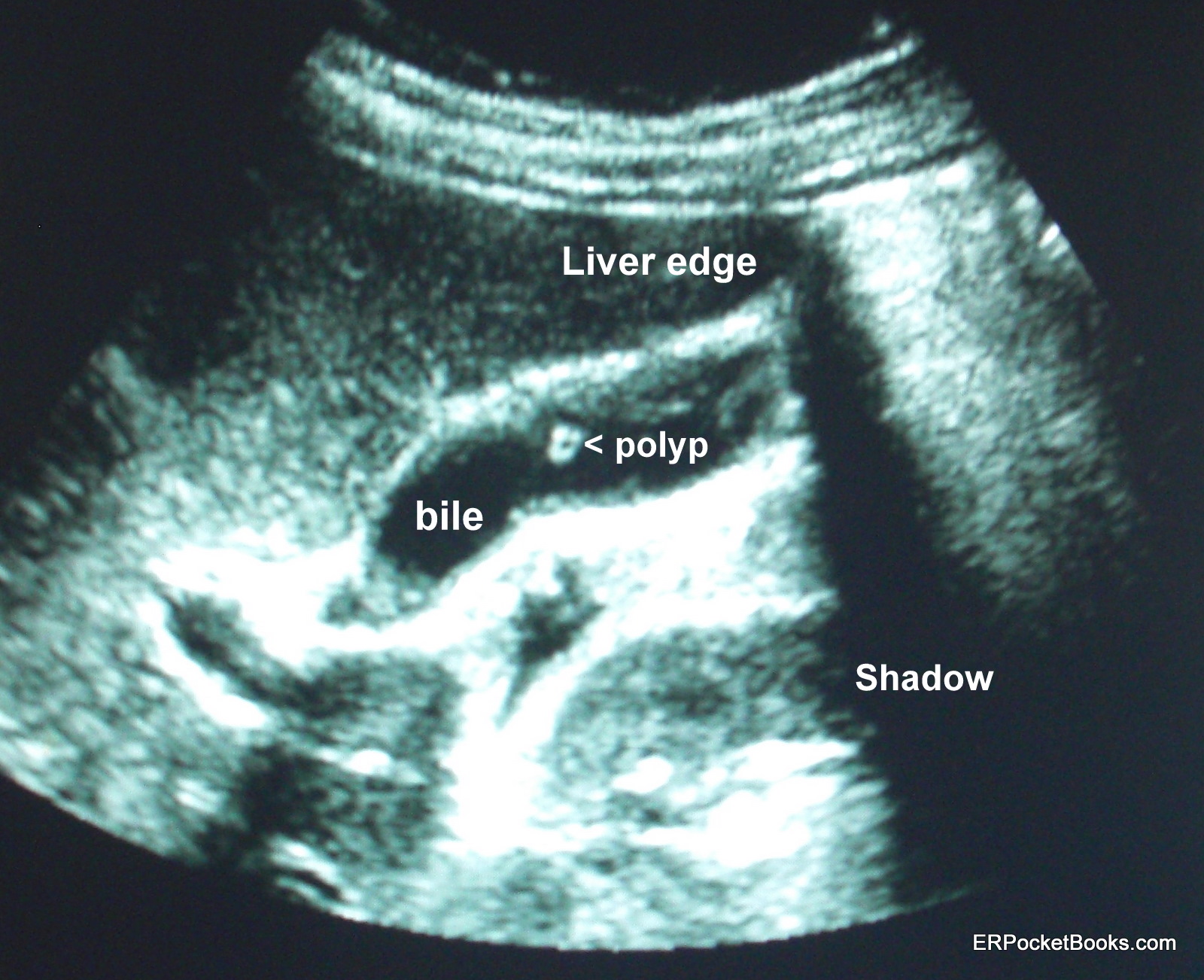
Gallbladder Polyp – Long Axis
****
WOULD YOU LIKE TO USE ONE OF OUR IMAGES?
As long as you paste the following statement with a weblink to this site, no problem: “Image reproduced with permission, ERPocketBooks.com”
****
this was very helpful to me as a new student learning about
ultrasound