PE Syndromes:
You will miss fewer PE’s if you know the PE Syndromes: Small, Classic and Large (which includes Sub-massive and Massive)
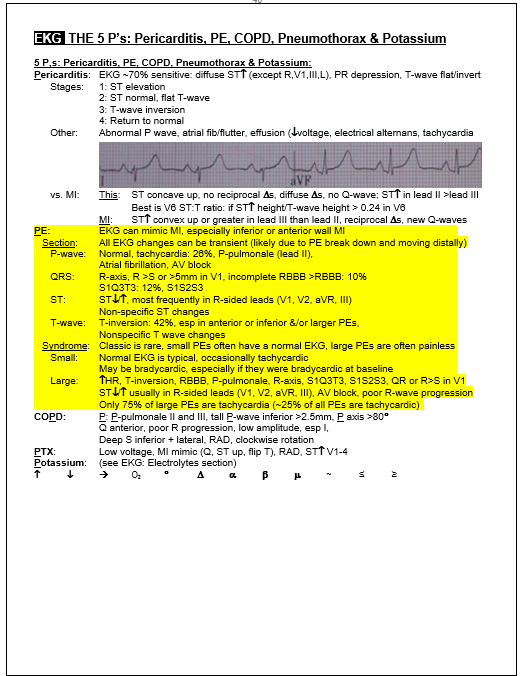
Small PE Syndrome: NO TACHYCARDIA. These PE’s lodge distally in the pulmonary circulation and so may cause peripheral lung infarcts. When symptomatic patients complain of pleuritic torso pain and sometimes cough or hemoptysis. Small PE’s may also be asymptomatic. The EKG is typically normal as are vitals signs, and lab work except the D-dimer.
Classic PE syndrome: This has all of the symptoms, signs and test results that you learned in medical school along with one or two obvious risk factors so that any medical student should be able to make the diagnosis. EKG findings are more typical of Large PE Syndrome.
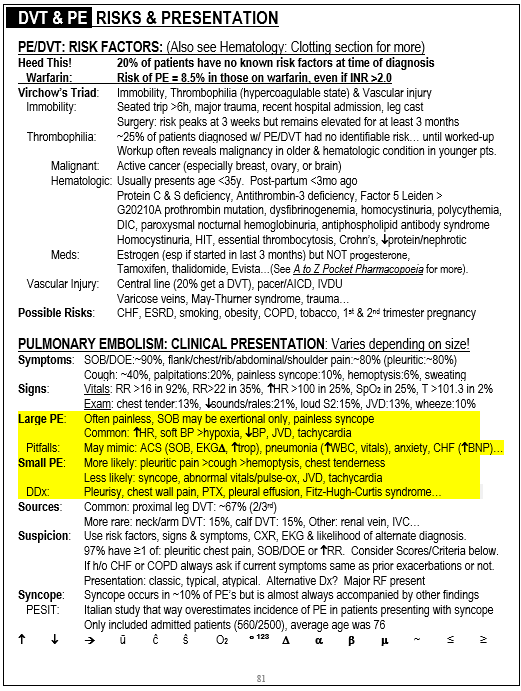
Large PE Syndrome: NO PAIN. Clinically patients present with dyspnea and/or near syncope. Chest pain is often absent because clots lodge proximally and so there is no lung infarct. There are often abnormal vital signs with tachycardia or a heart rate in the 90’s and sometimes hypoxia and/or hypotension. Large PE’s may mimic ACS with elevations of troponin and BNP due to right heart strain. They can also mimic sepsis with hypotension, tachycardia and elevated WBC count. The EKG is usually abnormal in one or more of the ways listed below.
PE EKG:
There is a lot of misunderstanding about EKG findings in PE. Many people think that most people with PE are tachycardic, when actually it is only about 25% in most of the more recent studies. The sample page below shows the top 5 EKG findings (the mnemonic is the letter T) and the more rare findings (the mnemonic here is the letter R)
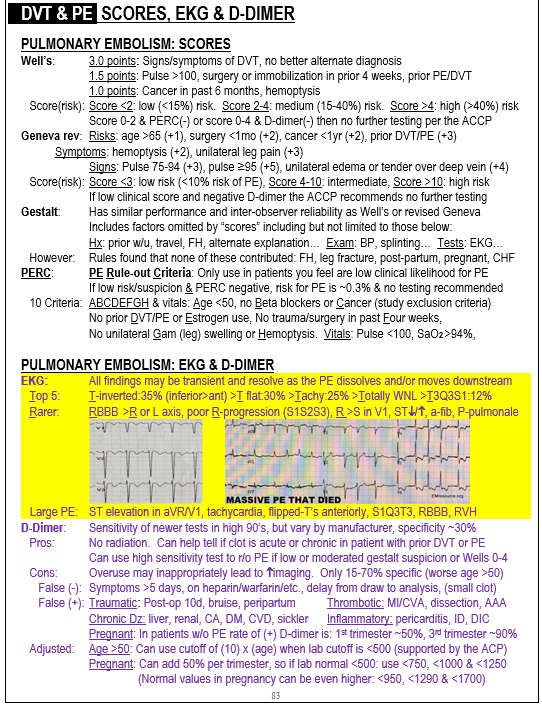
The PE section of the page-shot below is organized in 2 ways, first by the EKG section and second by PE size. Categorizing EKG findings by PE size is the most clinically useful. The same also applies to clinical symptoms (the “PE Syndromes” in the first part of this web-page).
****
DVT Mimics
Acute Limb Ischemia: Always check pulses. Pain here is typically distal but can be proximal, even buttock or groin pain. Pulses and warmth usually asymmetric so can detect with good exam, but this is not always the case so if high suspicion consider arterial vascular study or at least ABI’s.
Scitatica: Check DTR’s and strength including heel and tip toe gait.
Cellulitis: Feel for warmth
Nec Fasc: Feel for warmth
Pyomyositis: rare, but keep it in the differential if fever