History:
A patient in their mid 40’s with HTN and hypothyroidism comes to the hospital for RLQ pain for 2 days and cough for 1 week. She denies chest pain, SOB or N/V/D or any other complaints.
Vital Signs & Physical Exam:
Vital signs are normal. Physical exam is also normal except for RLQ and R mid-abdominal tenderness and fullness
Initial Diagnostic Testing:
- CBC: normal
- Chem-7: normal
- UA: 15 WBC and 1000 RBC
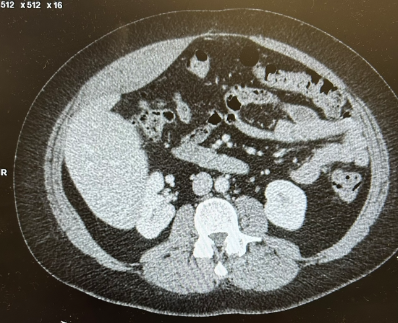
- Imaging: CT below
What is the most likely diagnosis?
- A) Appy
- B) Hematoma
- C) Kidney stone
- D) Pneumonia
SCROLL DOWN FOR ANSWERS & 1-MINUTE CONSULT
<<<<<<<<<<<<<<<<<<<<< ADVERTISEMENT & SPACER >>>>>>>>>>>>>>>>>>>>>
****************************************************************************
THE EMERGENCY MEDICINE POCKETBOOK TRIFECTA

Get one of our publications, all designed specifically for Emergency Care Providers:
Emergency Medicine 1-Minute Consult, 5th edition
A-to-Z EM Pharmacopoeia & Antibiotic Guide, NEW 5th edition
8-in-1 Emergency Department Quick Reference, 5th edition
******************************************************************************
***************************************************************************
<<<<<<<<<<<<<<<<<<<<<<<<< END SPACER >>>>>>>>>>>>>>>>>>>>>>>>>
ANSWER:
- A) Appy
- B) Hematoma – CORRECT – There is a rectus sheath hematoma on the right. The usual cause is coughing PLUS blood thinners. She only had the coughing, which is very unusual.
- C) Kidney stone
- D) Pneumonia – not seen on this cut but was seen on the CT though not on the CXR
CASE CONCLUSION: Vitals and serial Hb stable. Discharged home with doxycycline + Norco
1-Minute Consult on Rectus Sheath Hematoma
- Clinical: pain >swelling, surface bruising.
- Risks: cough, blood thinners
- Testing: CT
- Treatment: Analgesia/antitussives, reverse/hold thinners, (transfuse, embolize, OR)
***