Triage: CP x 4h, onset laying in bed, unable to sleep, gradual onset of pressure like, substernal radiates to L chest, nothing makes it worse or better, denies pain on inspiration or palpation, denies recent illness. Had 2 cocktails/1 beer last night
History: male in mid 40’s with no PMH presents with constant chest pain for past 8 hours radiating to his left shoulder and trapezius ridge as well as his upper interscapular area. He is not short of breath and the pain is not pleuritic per se but he said states it is difficult to take a full breath. Nothing else wakes it worse. No fever chills or history of same. No other complaints. FH: non-contributory.
Vital Signs: T: 36.2 °C (Oral) HR: 82 (Peripheral) RR: 15 BP: 135/74 SpO2: 98%
Exam: Normal peripheral pulse; normal heart and lung exam.
An ECG is done
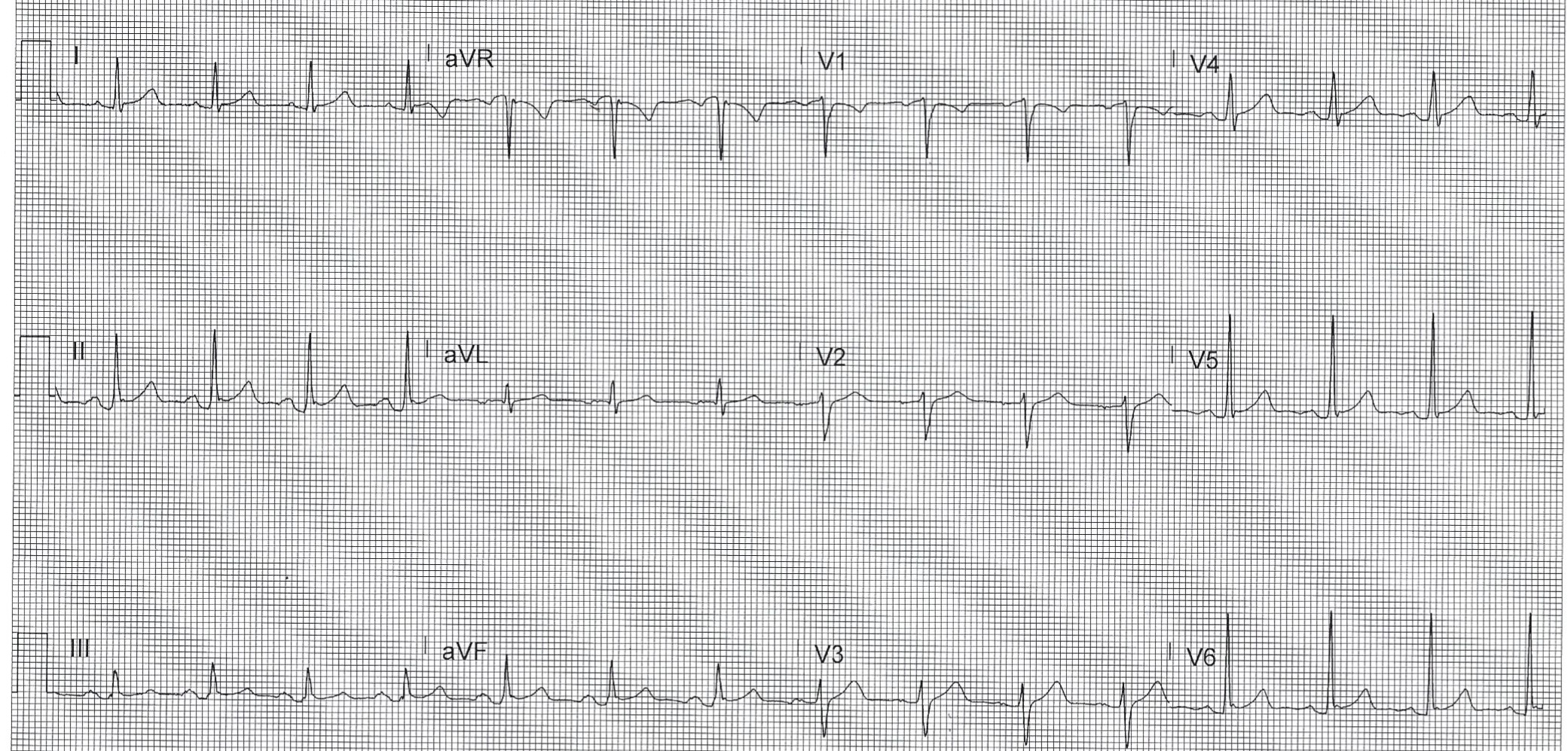
Computer read: NSR at 88, Early Repol
What is the most likely diagnosis?
- A) ACS
- B) PE
- C) Gastritis
- D) Anxiety
- E) None of the above
<<<<<<<<<<<<<<<<<<<<< ADVERTISEMENT & SPACER >>>>>>>>>>>>>>>>>>>>>
THE EMERGENCY MEDICINE POCKETBOOK TRIFECTA

- Emergency Medicine 1-Minute Consult, 5th edition
- A-to-Z EM Pharmacopoeia & Antibiotic Guide, 5th edition
- 8-in-1 Emergency Department Quick Reference, 5th edition
******************************************************************************
<<<<<<<<<<<<<<<<<<<<<<<<< END SPACER >>>>>>>>>>>>>>>>>>>>>>>>>
ECG interpretation: There is subtle diffuse ST elevation and PR depression most notable in inferior leads and in V4-V6. There is also a subtle Spodick’s sign mostly in these same leads
QUIZ ANSWER:
- A) ACS
- B) PE
- C) Aortic dissection
- D) Anxiety
- E) None of the above – CORRECT – Pericarditis is the most likely diagnosis, but as Steve Smith says, “Diagnose pericarditis at you patient’s peril” meaning you better be sure. Fortunately serial troponins and a CTA of the chest were negative for aortic dissection and ACS.
1-Minute Consult on this topic: Click HERE and scroll to proper page
Case Outcome: Trop x2 and CRP 4h after onset were normal as was CTA of the chest. Seen by cardiology who agreed with diagnosis of pericarditis. Discharged home on colchicine BID + ibuprofen prn. Next day CRP had risen from 0.10 to 4.22 and pain was milder overall but now worse supine.