Triage: BIBM from school pt c/o syncopal episode. Pt lowered self to ground, unconscious for 3 mins, minor shaking episode.
History of Present Illness: This is a 15-year-old female who was brought in by ambulance for a witnessed 3-minute generalized tonic-clonic seizure around 930 this morning with postictal period of about 5 to 10 minutes. Patient has no known history of seizure no warning or prodrome. She did recently increase her Wellbutrin from 300 mg a day to 450 mg a day approximately 4 days ago and was also started on Remeron at that time. She does recall leaving the scene but does not recall ambulance arrival after her seizure. Currently she feels tired but otherwise okay. She did have a stomach flu but that resolved about a week ago otherwise was feeling well earlier today.
Vital Signs: T: 36.9 °C (Oral) HR: 115 RR: 20 BP: 111/69 SpO2: 99%
Physical Exam: °EYES: Clear without discharge. No photophobia
°ENT: No oral trauma
°NECK: Supple
°HEART: Elevated rate. Regular.
°GENITOURINARY: No CVAT. No incontinence
°NEUROLOGIC: Normal speech. No focal weakness. Alert and oriented.
°PSYCHIATRIC: Normal mood. No SI
An ECG is done
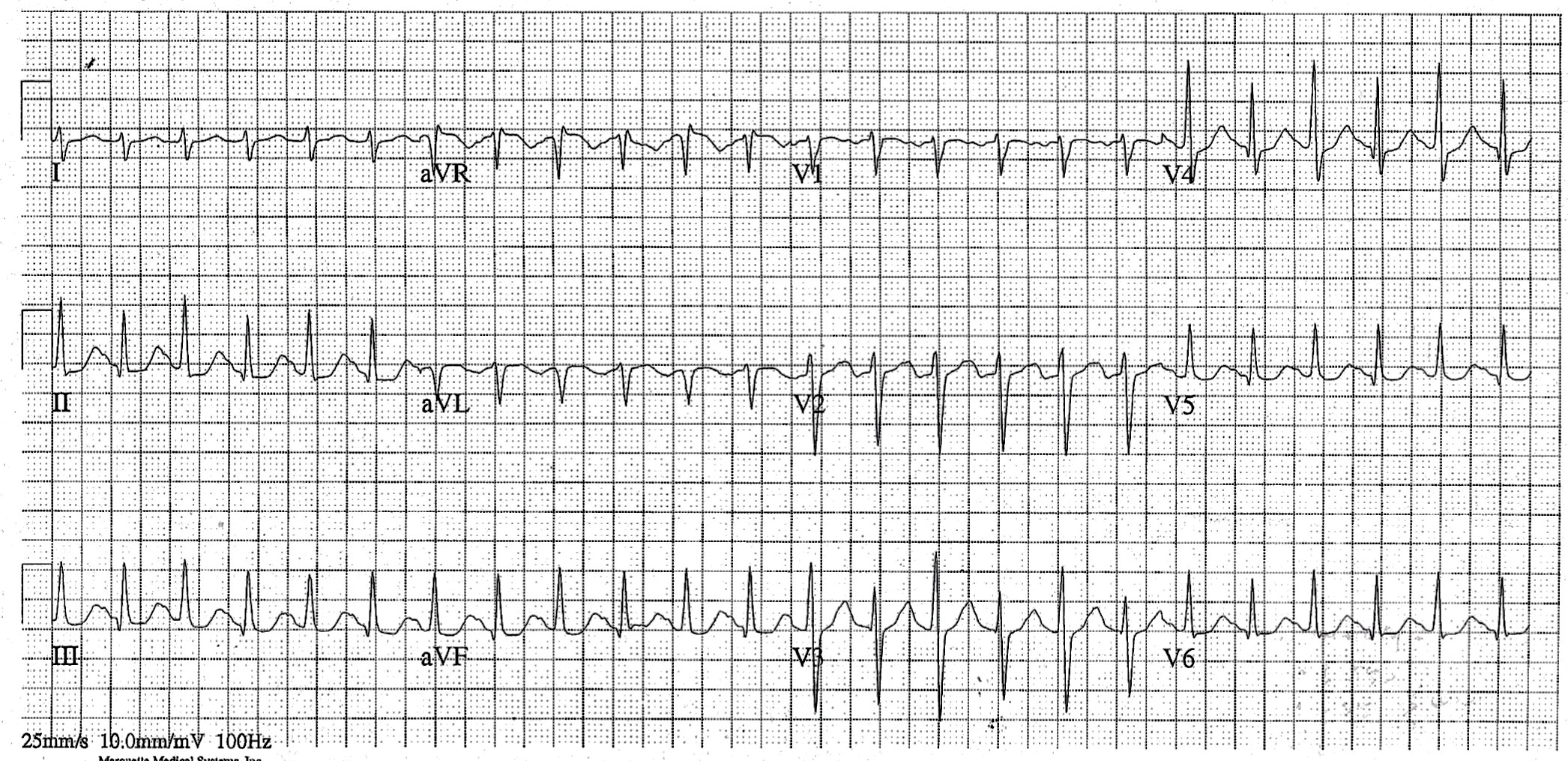
Computer Read: Sinus Tach at 141 w/ 1st degree AV block, Right axis, Nonspecific ST abnormality
What is the most likely cause of ECG findings in this patient?
- A) Normal
- B) Electrolyte issue
- C) Pulmonary embolism
- D) Drug toxicity
SCROLL DOWN FOR THE EKG ANALYSIS & 1-MINUTE CONSULT
<<<<<<<<<<<<<<<<<<<<< ADVERTISEMENT & SPACER >>>>>>>>>>>>>>>>>>>>>
THE EMERGENCY MEDICINE POCKETBOOK TRIFECTA

- Emergency Medicine 1-Minute Consult, 5th edition
- A-to-Z EM Pharmacopoeia & Antibiotic Guide, 5th edition
- 8-in-1 Emergency Department Quick Reference, 5th edition
******************************************************************************
<<<<<<<<<<<<<<<<<<<<<<<<< END SPACER >>>>>>>>>>>>>>>>>>>>>>>>>
ECG interpretation:
Interpretation: Computer read is accurate
QUIZ ANSWER:
-
- A) Normal
- B) Electrolyte issue
- C) Pulmonary embolism – Right axis and tachycardia should absolutely make you worry about PE. Even though the history was pretty clear that this was a seizure and not syncope and there was no chst pain or SOB, a D-dimer was sent, which was normal
- D) Drug toxicity – CORRECT – She had seizure and has persistent tachycardia from Wellbutrin toxicity. Other than Tramadol, Wellbutrin is probably the prescription medication most likely to cause seizure at usual doses.
1-Minute Consult on this topic: Click HERE and scroll to appropriate page
CASE CONCLUSION: CBC metabolic panel viral panel all essentially normal as was D-dimer, urinalysis and pregnancy test. Case discussed with children’s neurology who recommended no brain imaging. Patient remained persistently tachycardic with no definite cause even after IV fluids. Case discussed with poison control who recommended 24-hour admission. She did well, had resolution of tachycardia and no further seizures.